

Moms, you need to hear this: Just because breastfeeding is a natural process doesn’t mean it’s easy. Perhaps it’s a latch issue, a tongue-tied newborn, or just a sleepy baby: whatever the reason, women with difficulties breastfeeding often blame themselves. With the many changes new mothers face during this time, you’ll need to be reintroduced to the way your body sustains this fresh light in your life.
The more you know about yourself and your baby, the easier it will be to get past the bump (or bumps) in the road, so we’re here to help and offer solutions to common breastfeeding problems:
Insufficient Milk Supply
Mothers often stop breastfeeding because they believe they don’t have enough milk. In most cases, it’s a matter of perception, often caused by poor infant transfer of milk and/or poor latch; or by not feeding frequently enough, thereby down-regulating the milk supply. True cases of insufficient milk supply are rare, often related to a history of breast surgery (especially breast reduction surgery), hormonal imbalances, insufficient glandular tissue in the breast or no breast tissue changes during pregnancy, and consuming medications that interfere with breastmilk production.
Solution:
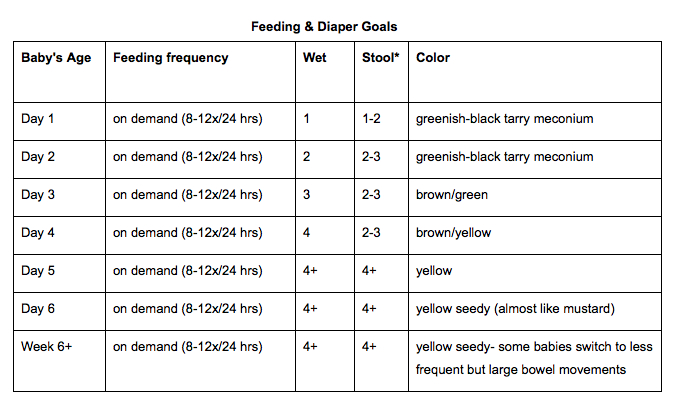
In this case, it’s important for mom to get the support of an IBCLC (International Board Certified Lactation Consultant) to maximize milk production and collaborate with the baby’s pediatrician to ensure adequate weight gain via breastfeeding and supplementation while protecting whatever supply mom has. Being attuned to your baby’s normal output (both pee and poop) and overall appearance is especially important during this time.
Nipple and Breast Pain
Sore nipples and/or breast pain often leads to a premature end of breastfeeding for a simple reason--it really hurts! This is a new experience for your body, so tenderness should be expected. Extreme or unbearable pain, however, requires the support of your healthcare provider or IBCLC to observe your breastfeeding and determine the cause and severity of nipple damage.
It’s important to understand the difference between “normal” nipple sensitivity and nipple injury based on occurrence and change over time. Keep in mind that nipple sensitivity normally increases during pregnancy and peaks about four days after giving birth. Combined with 8-12 nursing sessions per day and a poor latch and you have a recipe for damaged, painful nipples! Normal sensitivity typically goes away 30 seconds after suckling begins. Nipple pain caused by trauma, on the other hand, persists or gets worse after suckling begins. Severe pain or pain that continues after the first week following birth is more likely due to nipple injury.
Nipple Pain
Nipple Injury
Typical Cause:
Poor latch/position
Prevention:
Keep nipples dry between feedings. Avoid using harsh cleansers on nipples. Be sure to evaluate if your baby has mouth abnormalities.
Management:
Apply an ointment like our Organic Nipple Cream to raw and cracked nipples to help with healing. Cover with a nonstick breastpad to protect treated area from clothing.
Try warm or cool compresses if they reduce symptoms.
If your breast is too painful to feed your baby, use a pump or hand expression to remove milk for feeding and avoid engorgement.
Make sure to see your healthcare provider if the condition does not improve.
Plugged Milk Ducts
Leads to abrupt decrease in feeding, engorgement, and recurring infection.
Typical Cause:
Poor latch that leads to incomplete emptying of the breast. Wearing tight clothing or ill-fitting bra. Abrupt decrease in feeding, engorgement, and infections
Prevention:
Empty breasts of milk to prevent engorgement. Wear a properly-fitted bra. Ensure good latch.
Management:
Improve baby’s latch with the help of an IBCLC.
When baby is feeding, massage the plug gently towards the nipple. If plug or discomfort persists for more than 2-3 days, contact healthcare provider to determine other possible issues.
Nipple Vasoconstriction (Raynaud’s Phenomenon)
Typical Cause:
Tightened blood vessels in the nipple do not let enough blood through.
Prevention:
Feed in a warm environment.
Management:
Apply a warm compress on the nipple after feeding.
Breast Pain
Mastitis
An inflammation of the breast often associated with fever, muscle and breast pain, and redness.
Typical Cause:
Nipple infection or breasts being engorged for too long
Prevention:
Empty breasts regularly with a good latch.
Treat nipple infection if you have one (under direction of a physician).
If you have any of the following symptoms see a physician right away:
A firm, red, and tender area of the breast
Fever higher than 101˚F or 38.5˚C
Muscle aches, chills, malaise, or flu-like symptoms
Management:
Most women with mastitis will be prescribed antibiotics. Ask your doctor for a prescription that’s safe for breastfeeding. No need to pump and dump!
Empty your breasts frequently.
Work with an IBCLC on positioning and latch so that your breasts can be emptied more successfully and nipples can heal.
Help reduce swelling with cold compresses. Help increase milk flow with warm compresses in cases where milk stasis has occurred.
Oversupply
Typical Cause:
Unknown but more common in women having their first child.
Prevention:
There is no way to prevent it. Oversupply can be just as difficult as an insufficient milk supply (trust me, I was one of these mommies with both of my kids!).
In women with an oversupply of milk, the strong letdown of milk can cause the infant to choke, cough and have trouble feeding, or even to bite down to clamp the nipple. Infants whose mothers make too much milk can either gain weight quickly or gain too little weight because they cannot handle the flow of milk or because they do not get the “hindmilk,” which has the most calories.
Management:
Nurse in a laid back (biological position) to give the baby better control of the milk flow.
After milk lets down, you can remove baby from breast, put a burp cloth over your breast (if she is having difficulty) and wait for flow to slow down. Re-latch.
Pump very little or not at all because it can stimulate even more milk production. You can hand express a little at the beginning of a feeding to relieve some of the pressure.
Engorgement
Typical Cause:
Engorgement is the medical term for when the breasts get too full of milk. The fullness and firmness can cause pain and tenderness. Engorgement can sometimes impair the baby’s ability to latch, heightening symptoms and preventing the baby from emptying the breast.
Prevention:
Frequently empty breasts using a good latch. If you have difficulty, consult an IBCLC.
Management:
If engorgement makes it hard for your baby to latch on, manually express a small amount of milk before each feeding to soften your areola and make latching easier.
Apply warm compresses or take a warm shower before a feeding. This can enhance let-down and may make it easier to get milk out.
Avoid excessive pumping as it can stimulate even more milk production.
Special Circumstances
In all of these cases, there is also the chance the problem is due to the baby’s mouth structure or sucking ability. It’s important to have a feeding session observed by an IBCLC as well as a feeding specialist to determine what the issues are and develop a plan to help you reach your feeding goals safely.
Ankyloglossia (also called tongue-tie) is when the baby’s tongue cannot move as freely as it should, making it hard for the baby to suckle effectively.
Speak to your baby’s pediatrician for a referral to a lactation consultant and a pediatric ENT.
Torticollis is when the baby’s neck is twisted, making it hard for the baby to nurse from both breasts comfortably.
Ask your healthcare provider for the appropriate course of physical therapy.
Uncoordinated suck is when the baby does not move its tongue in the correct rhythm to pull milk from the breast.
Consult with your IBCLC to observe your breastfeeding.
Birth defects in the shape of the baby’s mouth may also make it hard for the baby to latch on (e.g., cleft lip/palate).
As treatment depends on defect and severity, please consult with your healthcare provider.
Remember that breastfeeding is a journey and you’ve got the most precious companion to accompany you on it. Do your best to enjoy the ups and the downs because this is one of the most intimate times you can have with your child.
-Nicole Meadow, MPN, RD, CSP, CLC
We wish you luck in reaching your personal breastfeeding goals for National Breastfeeding Month and beyond! Share your own journey in the comments below.
We aim to provide you with the most honest and credible information possible. This article was reviewed for accuracy by The Honest Team and was written based on sources that are linked at the bottom of the article.
blog_review_statement



{kind=link}
{kind=link}